*Please note: This slide show represents a visual interpretation and is not intended to provide, nor substitute as, medical and/or clinical advice.
Inflammatory bowel disease (IBD) encompasses a variety of disorders that cause inflammation of the digestive tract, including Crohn’s disease and ulcerative colitis.
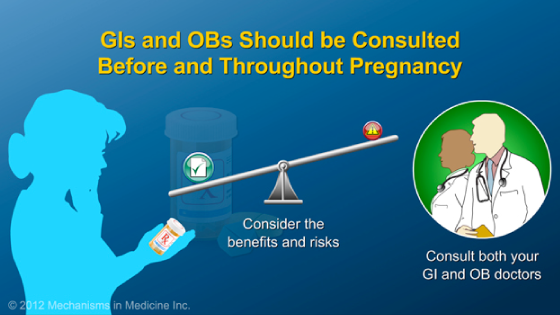
Active disease can pose health risks to either or both the mother and fetus if left untreated. Women trying to conceive should work with their doctors to have a healthy conception and pregnancy.
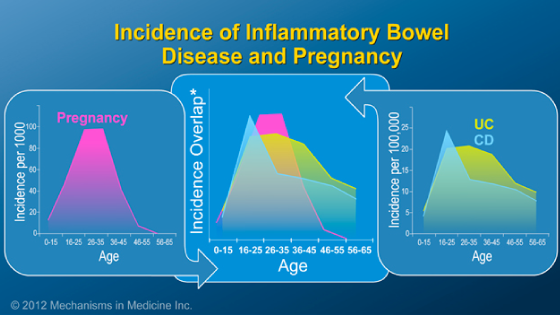
Women with IBD can typically become pregnant as easily as other women however those who have undergone a colectomy with ileal pouch anal anastomosis (IPAA) may have more difficulty due to the formation of adhesions or scarring on the fallopian tubes. Consult your obstetrician about fertility options if you are having trouble getting pregnant.
The state of IBD prior to conception can influence its progression during pregnancy. Remission at conception is critical to a healthy pregnancy outcome. About three-quarters of women in remission prior to becoming pregnant stay in remission during pregnancy.
Conversely, women with inadequately controlled IBD prior to conception are more likely to experience continued or worsened IBD activity during their pregnancy.
When a woman with IBD becomes pregnant, an obstetrician may recommend that some IBD treatments be stopped.
However, active disease poses the greatest risk to pregnancy, not the risk from IBD medications.
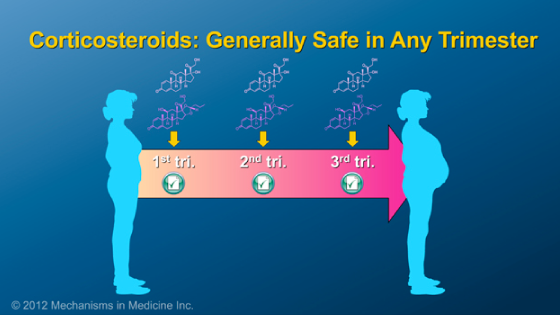
As a principle of IBD management, the maintenance of remission with medications is essential during pregnancy and should not be stopped in most cases.
Some medications, however, have risks for the fetus that clearly outweigh the potential benefits to the mother. Methotrexate and thalidomide fall into this category and should not be used during pregnancy.
All of the other medicines used to treat IBD are safe to take during pregnancy. It is important that you call your gastroenterologist before stopping ANY medicines.
Because active disease may pose risks to both the pregnant mother and developing fetus, appropriate steps should be taken to control IBD prior to and during pregnancy. Possible risks to the fetus when the mother has active disease include premature birth and low birth weight.
Pregnant women with IBD should discuss the ideal mode of delivery, C-Section versus vaginal delivery, with all of their doctors, including their obstetrician, gastroenterologist and their colorectal surgeon if they had surgery
Currently, the only contraindication to vaginal delivery is active involvement of the anal region due to Crohn’s disease or a previous history of severe disease in that area.
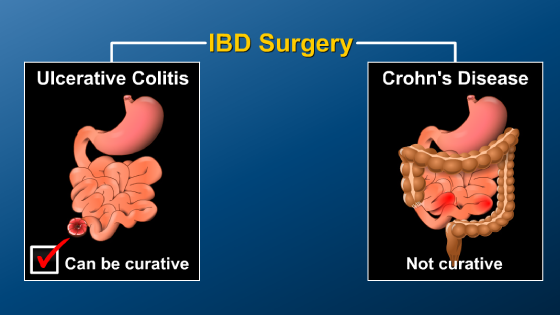
Most ulcerative colitis patients can deliver vaginally, but after colectomy, the preferred mode of delivery should be reviewed with the surgeon, obstetrician and gastroenterologist.
After giving birth, a woman may be concerned about the safety of breastfeeding while on medications to control IBD. Nearly all therapies used during pregnancy are safe to use while breastfeeding, although some antibiotics should be avoided. Please check with your doctor during pregnancy so you can feel comfortable staying on your medication during breastfeeding.
IBD itself does not impair fertility in males; however, some medications used to manage IBD may decrease male fertility. The sperm of males taking sulfasalazine may have impaired motility and abnormal shape or number. However, infertility due to sulfasalazine is temporary and can be reversed when the medicine is discontinued.
While IBD does not represent a significant barrier to becoming pregnant, health risks are imposed on both the mother and developing fetus if IBD is left untreated. By taking appropriate steps to achieve remission prior to conception and continuing therapeutic drug treatments throughout pregnancy, the likelihood of a healthy pregnancy and delivery can be optimized.
This slideshow describes issues females with IBD should consider before getting pregnant. The fertility of patients with IBD and healthy people is compared, and the ways in which IBD may affect a pregnancy are described. The slideshow emphasizes the need to establish remission before becoming pregnant and to maintain remission during pregnancy by using safe medications. Finally, the topic of whether it is safe to breastfeed while taking IBD medications is addressed.
-
Share with family and friends:
Click here to take our SURVEY
Your feedback is important to us! We will use your feedback to develop future areas of content about IBD which will help other patients, caregivers and families.