Please note: This slide show represents a visual interpretation and is not intended to provide, nor substitute as, medical and/or clinical advice.
Patients can prepare themselves for inflammatory bowel disease (IBD) therapy by understanding the risks of untreated or under-treated IBD, learning about the risks and benefits of the therapy, and being aware of the side effects associated with the treatment.
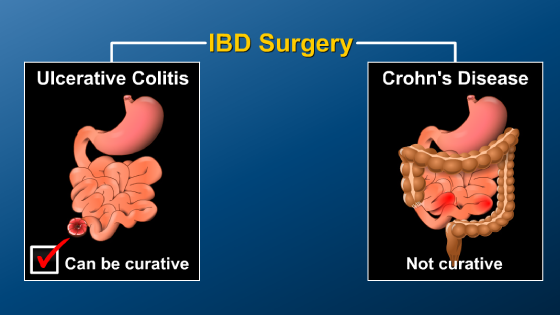
Patients should understand the risks of untreated or under-treated IBD. For some types of Crohn’s disease, no treatment or inadequate treatment can increase the likelihood of needing surgery to as high as 70% within 10 years.
Therapy can help to establish and maintain disease control, reduce the frequency of relapse, improve a patient’s quality of life, and in children, facilitate normal growth and development.
Patients can prepare for their IBD therapy by understanding risks and benefits of medications. Potential benefits of therapies for IBD include control of inflammation, improvement of symptoms, improvement in quality of life, prevention of relapse, reduction in complications of IBD, and reduction in the chance of requiring surgery. On the other hand, potential risks include short-term side effects, long-term toxicity, and the cost of the therapy.
Patients should discuss the risks and benefits of their therapy with their physicians. It is important to consider the risks and benefits of therapy compared to the risks of untreated disease.
Reliable web sites can also provide useful information, for example YouandIBD.com
Ask your doctor for other reliable sources.
Depending on the therapy used to treat IBD, patients may need to undergo tests to ensure that the medication is not affecting different parts of the body.
For example, although 5-aminosalicylates (which are known as 5-ASAs or mesalamines) are considered extremely safe and very effective to reduce colonic inflammation, it is recommended to have blood or urine tests of kidney function at least annually.
Although sometimes medically necessary, steroids are associated with many side effects, so patients on steroids (even short-term) should communicate with their doctor to determine if blood pressure, blood sugar, bone density, and other tests are required.
Immunomodulators such as 6-mercaptopurine, azathioprine, and methotrexate are considered quite effective and overall safe, patients on immunomodulators should have blood tests every few months and protect their skin from excessive sun exposure due to an increased risk of non-melanoma skin cancers
With azathioprine and 6-mercaptopurine, some of these risks are minimized by checking the activity of a genetically determined enzyme (TPMT) prior to starting therapy. This assessment allows for dosing and discussions of benefits and risks that are individualized for the patient.
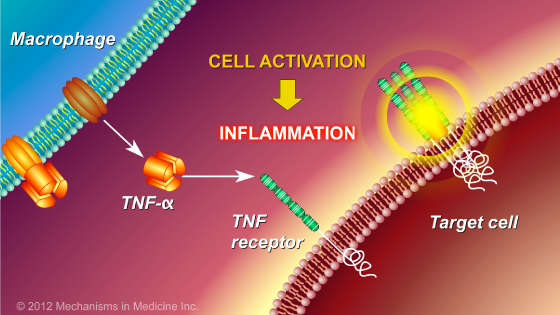
Biologics, such as anti-TNF therapy, have been shown to be the most effective way to treat some types of IBD and overall are considered quite safe.
However, patients should inform their doctors if they have had prior exposure to tuberculosis, a history of multiple sclerosis or optic neuritis, or severe congestive heart failure.
Before starting on anti-TNF therapy, patients need to be tested for tuberculosis and to see whether they have immunity to the hepatitis B virus.
This is important because if present, latent tuberculosis or chronic hepatitis B infection can worsen or reactivate due to the anti-TNF therapy.
The doctor should also take a history about vaccinations and check to see whether the patient has immunity to the varicella zoster virus, which causes chicken pox. Immunity to varicella zoster virus may be from prior infection or from prior vaccination.
If a patient does not have immunity to the chicken pox virus, a vaccine can be given prior to starting anti-TNF therapy.
The timing between getting the vaccine and starting therapy needs to be discussed with your doctor.
Reactivation of varicella zoster is known as shingles, and can happen with biologic therapies if immunity is not adequate.
Patients should know that smoking cigarettes might reduce the efficacy of anti-TNF therapy, and therefore patients should be encouraged to quit smoking and get help to do so if necessary before beginning therapy.
Effective communication between patients and their doctors can prevent adverse events with therapy.
In addition, patients should be up-to-date on all of their cancer screening and recommended vaccinations to prevent infections while on therapy.
Patients should discuss their immunization record with their doctors to determine which, if any, vaccines they should receive and when they should be given.
A bacteria known as Streptococcus pneumonia is a common cause of pneumonia, and can cause other infections.
It is recommended that children and adults with IBD should receive the pneumococcal vaccine. This vaccine is only given every 5 years.
Some patients should receive the hepatitis B vaccine, including health care workers, people who engage in high-risk behaviors, those who have had multiple blood transfusions or tattoos, and anyone who wants to receive the vaccine.
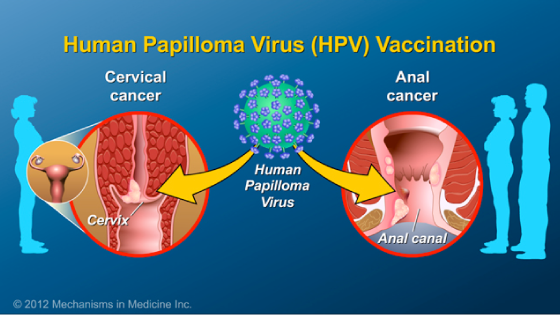
Human papilloma virus, which is also known as HPV, is sexually transmitted and has been linked to cervical cancer in women and anal cancer in men and women.
It is recommended that women and men with IBD who are under 26 years of age should receive the HPV vaccination, regardless of whether they are immunosuppressed.
Live virus vaccines, such as yellow fever, measles-mumps and rubella (MMR), rotavirus, and nasal influenza, should not be given to patients on immunosuppressive therapies, including those on steroids greater than prednisone 20 mg/d, azathioprine or 6-mercaptopurine (6-MP), methotrexate or biologics.
However, non-live influenza vaccines via injection are available for these patients.
Patients can prepare for IBD therapy by learning about the side effects that are associated with their treatment choice. By understanding the possible side effects of their therapy, patients can take steps to prevent them.